Pediatric Traumatic Brain Injury (GCS <8)
TBI Management Guideline
Neurologic Monitoring:
- Clinical – obtain baseline neurologic examination and Glasgow Coma Scale score (GCS) before sedation and muscle relaxants are administered
- Routine nursing neurovitals assessment hourly
Spinal precautions:
- Head of bed elevated 20-30° with head in neutral midline position, maintaining spinal precautions
- Semi-rigid cervical collar (Aspen) maintained until cervical spine cleared
Hemodynamic support:
- Maintain mean arterial pressure upper end of normal based on normal age range
Image
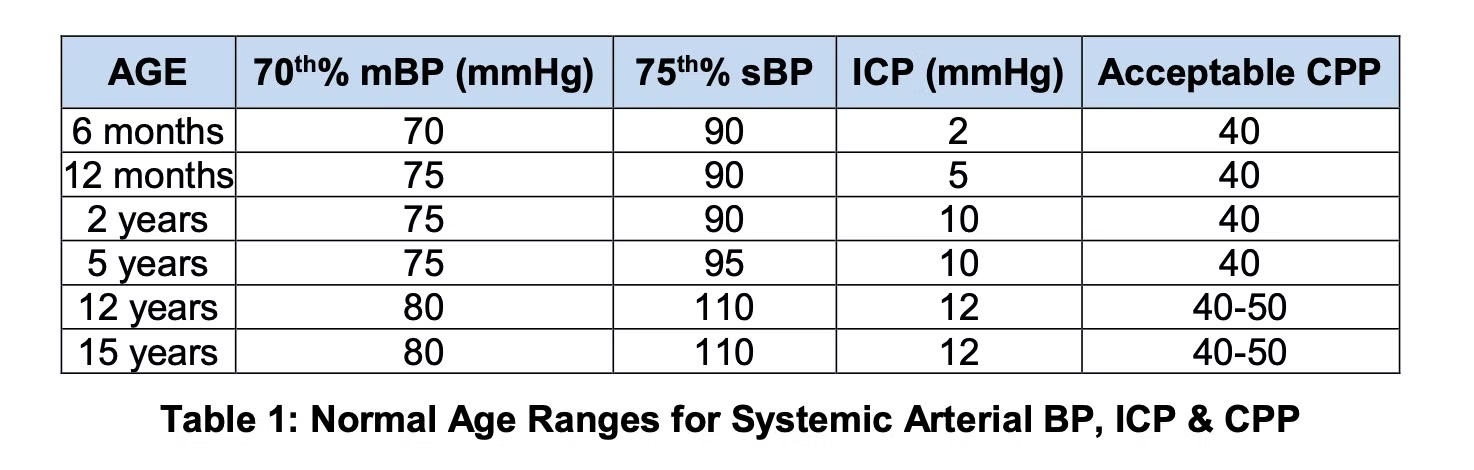
- Inotropes as required/fluids as required
Ventilation & Oxygenation:
- Maintain PaCO2 35 to 40 mmHg
- Wean FiO2 to maintain arterial saturations >94%
Fluid and electrolytes monitoring:
- All patients with brain injury (anoxic or traumatic) are at risk for disordered sodium regulation
- Early detection of sodium abnormalities is essential to maintaining serum sodium within target range and preventing secondary brain injury.
- D5W 0.9%NaCl at 70% maintenance
- Foley catheter and hourly urine output measurement for 48 hours
- Monitor serum electrolytes and blood gases every 6 hours for 48 hours – serum Na to maintain 140 or above
- Initial labs should include liver “function” and coagulation screen
- Maintain serum glucose 5-8mmol/L
- Notify PICU physician if urine output is < 0.5 mL/kg/hour, > 4 mL/kg/hour in a single hour, or > 2.5 mL/kg/hour for more than three hours
Temperature control:
- Monitor core temperature - esophageal (if available)
- Regular acetaminophen 15mg/kg NG/NJ every 6 hours – review every 24 hours
- Normothermia 36-36.8°C
- Consider neuromuscular blockade to facilitate temperature control
Sedation/analgesia:
- Initiate analgesia and sedation with morphine infusion 10-40 mcg/kg/hour and midazolam
infusion 50-150 mcg/kg/hour
Seizure prevention:
- Prophylactic levetiracetam (Keppra®) 10mg/kg NG/PO every 12 hours for 7 days
- For clinical seizures, give a loading dose of levetiracetam (60mg/kg IV)
- Consider EEG within first 36 hours of admission
- Continuous EEG monitoring is recommended if resources are available
Drs. Peter Skippen, Ash Singhal, Mandeep Tamber, Mary Connolly, Linda Huh. MANAGEMENT OF TRAUMATIC BRAIN INJURY IN CHILDREN WITH GCS < 8. [Internet]. 2021. Available from: https://shop.healthcarebc.ca/phsa/BCWH_2/Pharmacy,%20Therapeutics%20and%20Nutrition/C-05-07-62754.pdf