Before Intubation in Trauma
- RESUSCITATE before intubate
- Maintain C-Spine immobilization during intubation if C-Spine injury suspected
BCCH Child & Youth Health Policy and Procedure Manual. INTUBATION IN PEDIATRIC TRAUMA GUIDELINES [Internet]. Available from: https://shop.healthcarebc.ca/phsa/BCWH_2/BC%20Children%27s%20Hospital/C-05-07-62394.pdf
Assessment
The patient should be adequately assessed before and during intubation (airway examination, breathing examination)
BCCH Child & Youth Health Policy and Procedure Manual. INTUBATION IN PEDIATRIC TRAUMA GUIDELINES [Internet]. Available from: https://shop.healthcarebc.ca/phsa/BCWH_2/BC%20Children%27s%20Hospital/C-05-07-62394.pdf
Positioning
- The patient should be kept in NEUTRAL head position.
- The cervical spine collar should be removed during the intubation procedure, while maintaining manual in-line cervical spine precautions
Equipment
Personal Protective Equipment (PPE)
- Mask
- Eye Protection
- Gown
- Gloves
Monitoring Equipment
- pulse oximetry
- non-invasive blood pressure monitoring (either automated or manual)
- cardiac monitor
- End Tidal CO2 (ETCO2) or if unavailable use a colorimetric device
Airway Equipment
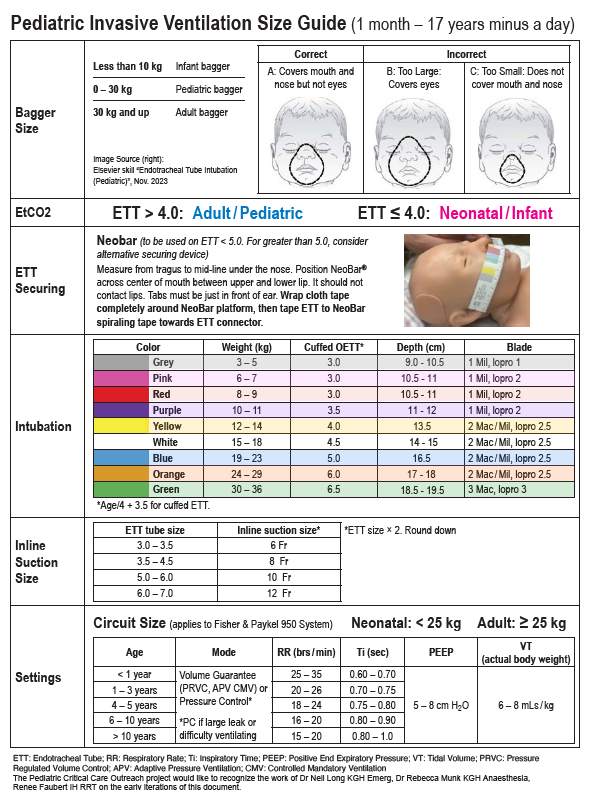
A cuffed ETT is recommended in Pediatric Trauma patients (including burns).
- The estimate for the tube size is:
- CUFFED ETT = age / 4 + 3.5
- UNCUFFED ETT = age / 4 + 4
- A Microcuff brand endotracheal tube (Kimberley-Clark) or Satin-slip stylet by Mallinckrodt are recommended
- Rigid suction system (Yankaeur)
- Pediatric Laryngoscope: Miller/Wis/Robertshaw (straight Blade) or Macintosh (Curved blade).
- Miller laryngoscope blades/Robertshaw laryngoscope blades (preferably fibreoptic) recommended
- Semi-rigid stylet (for endotracheal tube), lubricated with any water based lubricating jelly. Satin-slip stylet by Mallinckrodt is recommended
Checklist
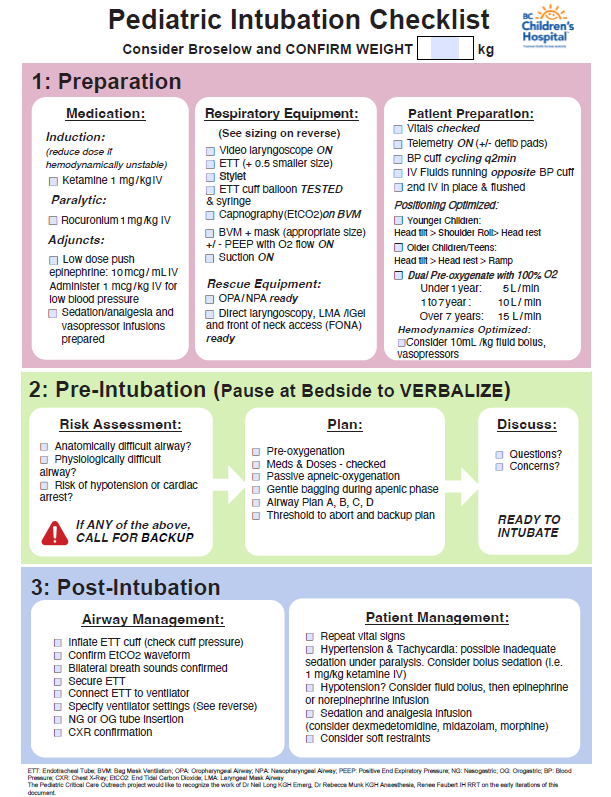
Long N, Munk R, Faubert R. Pediatric Intubation Checklist [Internet]. BC Children’s Hospital; Available from: https://www.childhealthbc.ca/media/1036
Pre-Oxygenation
- Prior to every intubation attempt, the patient should be maintained with oxygen via nasal prongs ( <1 yr = 5LPM, 1-7 yr = 10LPM, > 7 yr = 15 LPM) , in addition to 100% oxygen via bag-valve-mask (tight anatomical seal). This should be maintained while preparing equipment and medications
- If the face mask seal is impaired by the nasal prongs, remove the nasal prongs and optimize bag mask ventilation/oxygenation
- Ventilation should be supported if the patient is apneic or hypoventilating while preparing for intubation
Fluids
Ensure simultaneous effort to support intra-vascular volume using either an isotonic crystalloid solution or blood product depending on the clinical situation
Medication
If the weight is not immediately known or easily estimated, a Broselow tape can be used for the purpose of drug dosages (as well as ET tube sizing)
- Ketamine 1mg/kg
- Rocuronium 1mg/kg
- Vasopressors: Hypotension adversely affects outcome of children with traumatic brain injury. Hypovolemia and positive pressure ventilation may result in hypotension during the intubation procedure. If the patient is unstable at induction, anticipate problems and have a VOLUME and vasopressors available in case of further instability following the administration of anesthetic and institution of positive pressure ventilation
- Low Dose Epinephrine Push - 0.001mg/kg = 1 mcg/ml as required.