Diagnosis
Diabetic ketoacidosis (DKA) is diagnosed when:
- Blood glucose is >11 mmol/L
- Capillary pH is <7.3 and/or capillary bicarbonate is <18 mmol/L
- Ketones are present in the blood and/or urine
Hyperglycemic hyperosmolar state (HHS) should be suspected when:
- Hyperglycemia (>33 mmol/L) extremely high blood glucose levels, a hallmark of HHS.
- Hyper-osmolality (>330 mOsm/L) elevated serum osmolality, which reflects significant dehydration and concentration of solutes due to hyperglycemia.
- Little to no ketoacidosis
Mixed picture of DKA and HHS is possible
BCCH Endocrinology Department - Endocrinologist. DIABETIC KETOACIDOSIS MEDICAL PROTOCOL [Internet]. 2024. Available from: https://shop.healthcarebc.ca/phsa/BCWH_2/BC%20Children%27s%20Hospital/C-05-13-60395.pdf
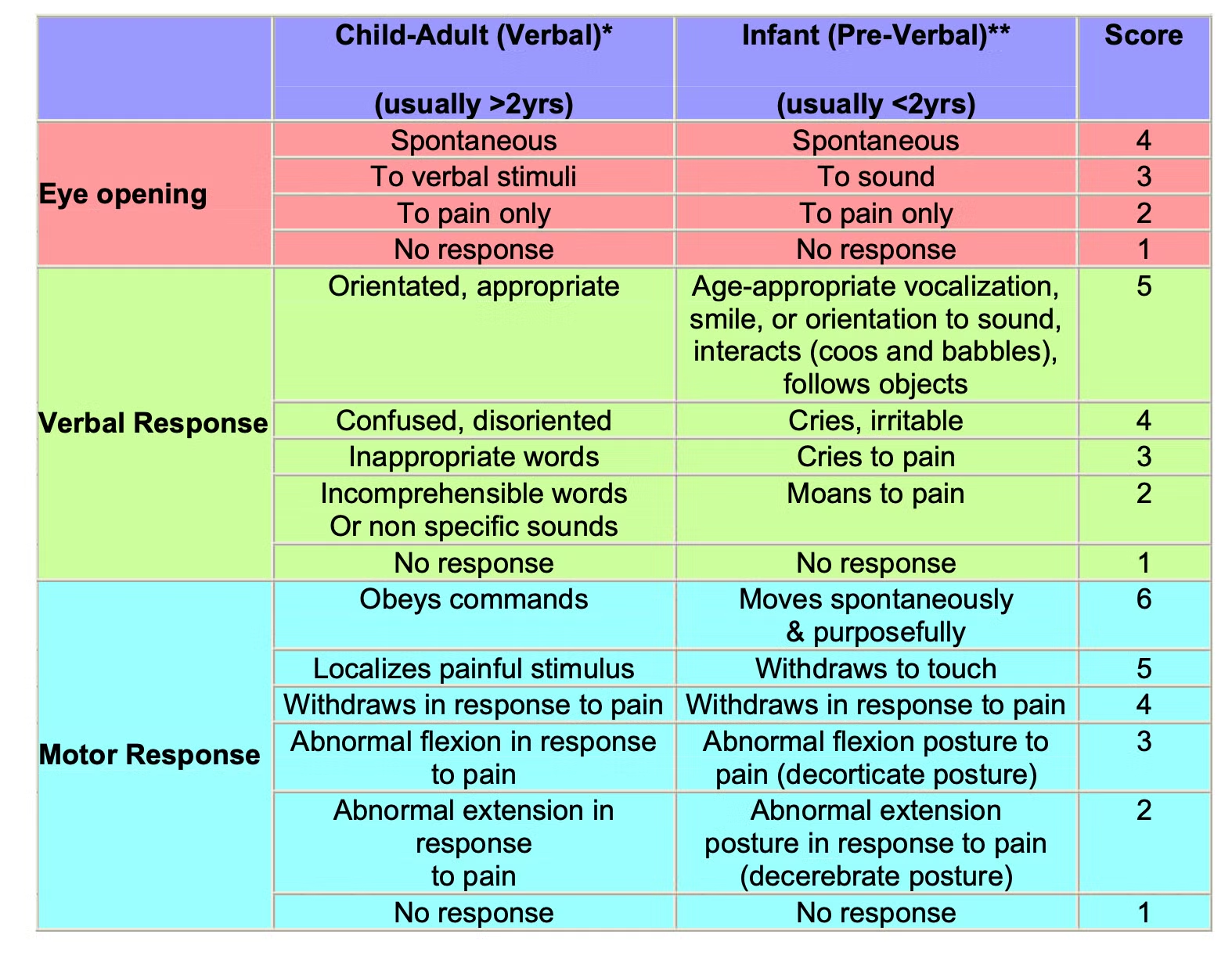
Neurological Observation in DKA
Follow Glasgow Coma Scale
Image
- Severe headache, change in sensorium or BP, dilated pupils, bradycardia, irregular
breathing, posturing and incontinence are signs of impending deterioration.
Rapid intervention is imperative:
- Airway / breathing / circulation
- Elevate head of bed
- Decrease all fluid bags to 5 mL/h pending physician reassessment
- Mannitol 20% (0.5–1 g/kg, 2.5–5 mL/kg IV over 15 min) or NaCl 3% (2.5–5 mL/kg
IV over 15 min) - Consider intubation and mild hyperventilation (keep pCO2 >22 mg Hg) for
impending respiratory failure - Arrange CT when stable
BCCH Child & Youth Health Policy and Procedure Manual. APPENDIX A: MODIFIED GLASGOW COMA SCALE (GCS) FOR INFANTS AND CHILDREN [Internet]. Available from: https://shop.healthcarebc.ca/phsa/BCWH_2/BC%20Children%27s%20Hospital/C-05-14-62116.pdf