Fluid Management
- TIME ZERO IS TIME OF INJURY
- Parkland/Modified Brooke Formula: Patient Weight (kg) x (%TBSA) x 3 mL
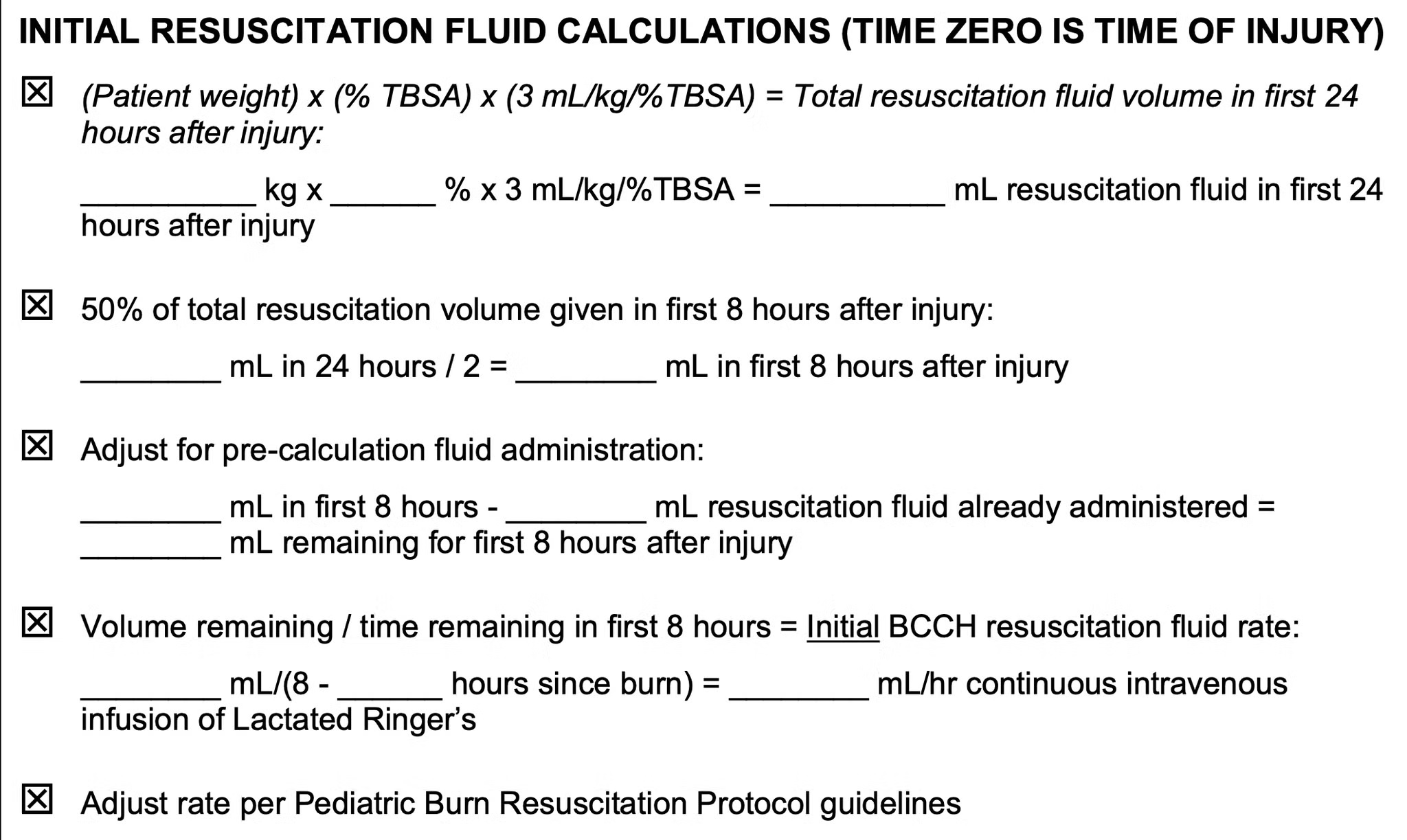
- Example: 24kg child with 50% TBSA burned:
- 24kg x 50% TBSA x 3 = 3600mL Ringer's Lactate resuscitation IV fluid required in the first 24 hours post burn
- Give 1800 mL in first 8 hours at 225 mL/hr, followed by remaining 1800 mL at 112 mL/hr over next 16 hours
- For children <30kg, add D5 NS MAINTENANCE IV fluid calculated with the 4:2:1 rule.
- For a 24kg child, they would receive 64mls/hr D5 NS MAINTANCE in addition to Ringer's Lactate resuscitation fluid
- Adjust Ringer's Lactate rate to target urine output of 0.5-1ml/kg/hr (12-24mls/hr in this example)
The University of British Columbia Division of Plastic Surgery. PEDIATRIC BURN REFERRALS [Internet]. Available from: https://www.ubcplastics.ca/copy-of-adult-burns
Burn Resuscitation Protocol (First 48 Hours)
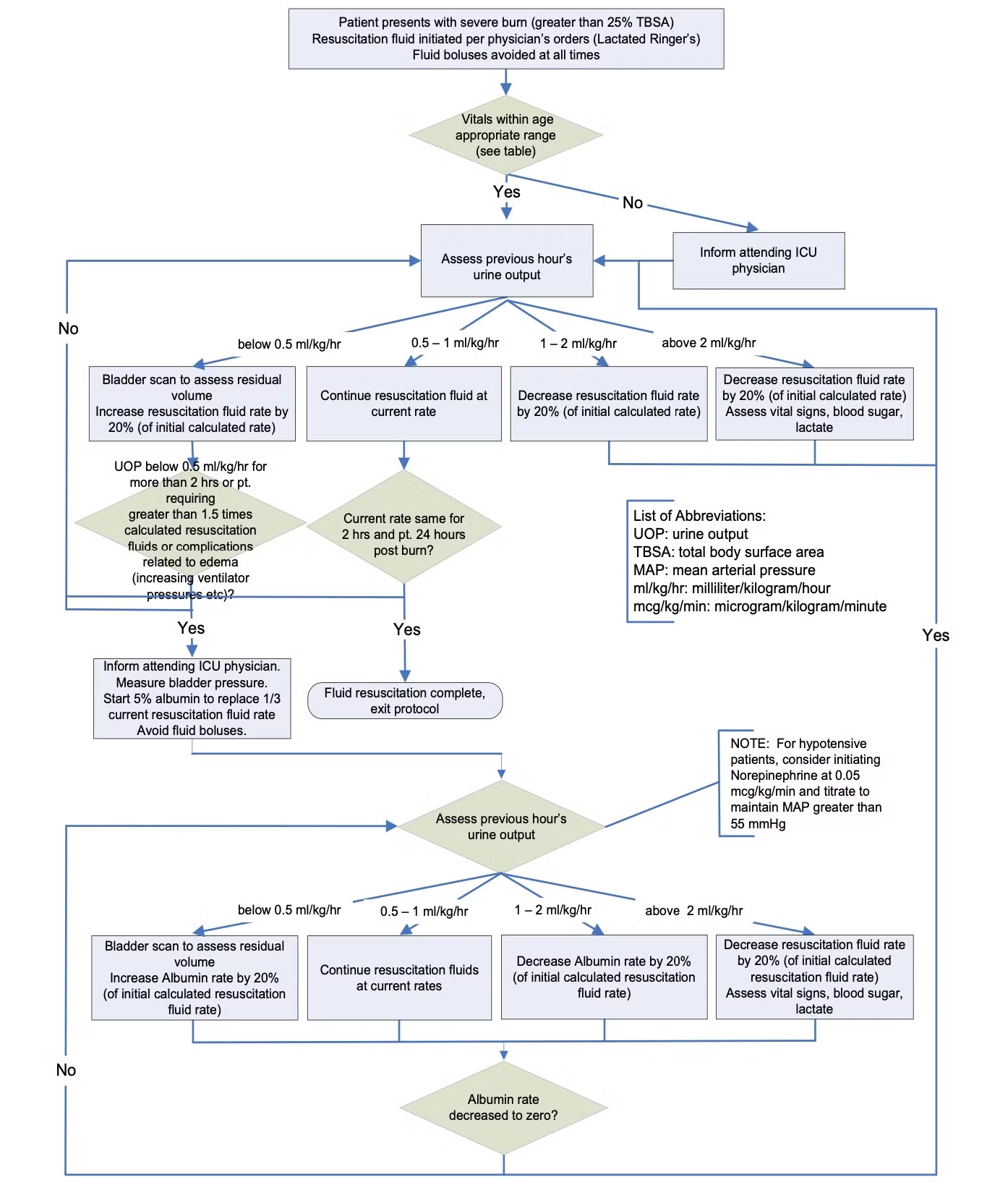
BCCH Child & Youth Health Policy and Procedure Manual. BURN RESUSCITATION PROTOCOL – INITIAL 48 HOURS [Internet]. Available from: https://shop.healthcarebc.ca/phsa/BCWH_2/BC%20Children%27s%20Hospital/C-05-01-62281.pdf
Management of Hypotension
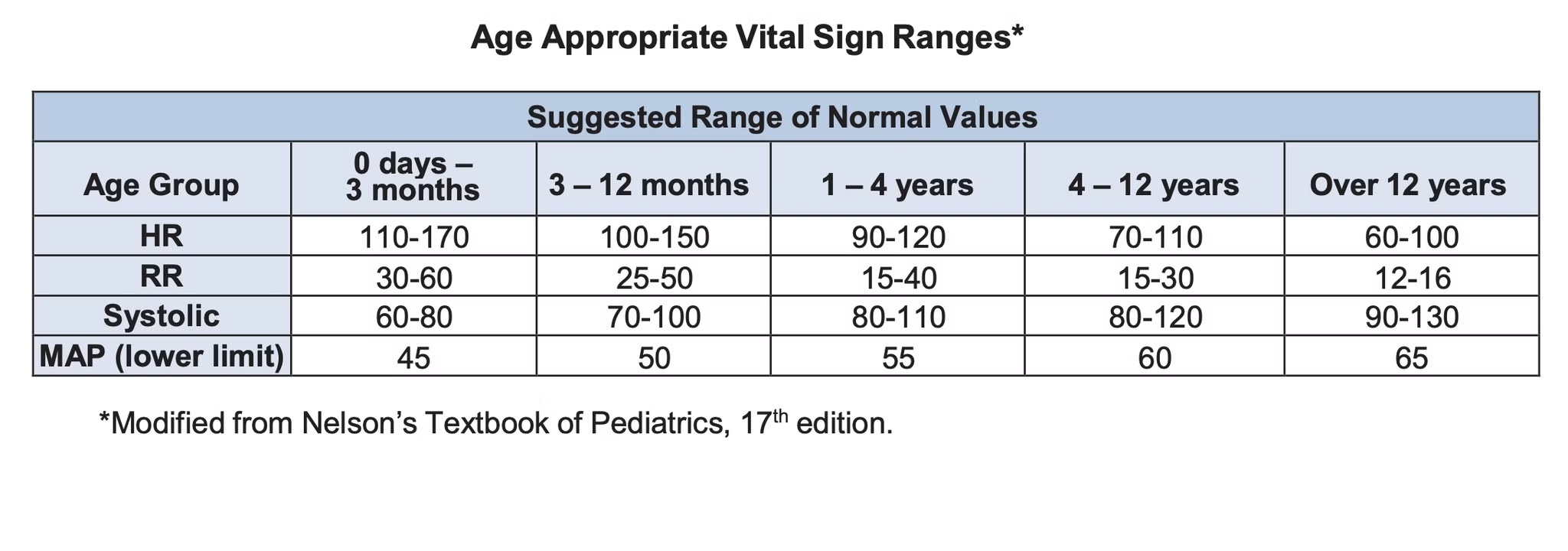
- Hypotension MUST NOT be defined or acted upon by MAP values alone. It must be correlated with decreased urine output and an overall patient assessment. MAP values less than those outlined in the table above are acceptable as long as urine output exceeds 0.5 mL/kg/hr, ScvO2 greater than 60% and lactate less than 3mmol/L
- Fluid boluses should ONLY be administered for the reversal of acute profound hypotension.
The following stepwise guide is recommended IF Mean Arterial Pressure (MAP) is consistently less than the lower limit for age and there is evidence of poor end-organ perfusion :
- Urine output less than 0.5 mL/kg/hr
- Lactate greater than 3mmol/L
- ScvO2 less than 70%
- Assess Volume Status: If MAP is less than the lower limits outlined above, CVP is less than 5 and urine output is below 0.5 mL/kg/hr, refer to the [Burn Resuscitation Algorithm](https://shop.healthcarebc.ca/phsa/BCWH_2/BC%20Children%27s%20Hospital/C-05-01-62281.pdf) to determine the appropriate increase in resuscitation fluid rate (generally 20%). Continue fluid administration as guided by the Burn Resuscitation Algorithm
- If MAP is persistently less than the lower limit for age and resuscitation fluid rate is greater than 2 times the initial calculated rate, consider initiation of Norepinephrine at 0.01-0.05 mcg/kg/min to maintain MAP above the lower limit for age (severe burn patients may require Norepinephrine for vasodilatory shock secondary to a massive systemic inflammatory response)
- Reassess Patient: If persistently requiring Norepinephrine (0.01-0.05 mcg/kg/min) consider a
lower MAP goal as long as urine output exceeds 0.5 mL/kg/hr, ScvO2 greater than 60% and
lactate less than 3mmol/L - Maintain ionized calcium greater than 1mmol/L
BCCH Pediatric Intensive Care Unit - Quality & Safety Leader. PICU SEVERE BURNS: VITAL SIGNS AND HYPOTENSION MANAGEMENT. 2021 https://shop.healthcarebc.ca/phsa/BCWH_2/BC%20Children%27s%20Hospital/C-05-14-62757.pdf
Burn Dressings
For ALL burn dressings consider sedation/pain management and appropriate monitoring. Psychological, physical, and pharmacological strategies can help to reduce discomfort and distress associated with procedures; overall this can promote comfort and improve the healthcare experience and quality of life for the child and family.
For BCCH recommended dressings refer to Pediatric Burn Dressing, Quick Reference Guide.