Recognition
Acute onset of skin changes (urticaria, erythema/flushing and/or angioedema) AND at least one of the following:
- Respiratory +/-
- Cardiovascular +/-
- GI symptoms
OR - Hypotension, bronchospasm or upper airway obstruction after exposure to known or highly probable allergen
TREKK. Pediatric Anaphylaxis Algorithm [Internet]. 2025. Available from: Trekk - Anaphylaxis Algorithm.
Management
0 to 5 MINUTES
- Place patient in supine position
- Assess ABCs, vital signs
- Provide O2 10-15 L/min by non-rebreather mask
- Identify and remove allergic trigger, if possible
- ADMINISTER IM EPINEPHRINE
DO NOT delay IM EPINEPHRINE administration
- Dose: 0.01mg/kg (1mg/ml), MAX 0.5mg
- Route: INTRAMUSCULAR (IM) in anterolateral thigh
- Never administer the IM preparation of epinephrine (1mg/mL) through IV/IO route
- Never give IV epinephrine bolus dose for initial anaphylaxis management, consider IV epinephrine infusion if no response after 3 doses of IM epinephrine
- REPEAT IM EPINEPHRINE every 5-10 min as needed (see below)
5 TO 10 MINUTES
Respiratory symptoms:
- Sitting position
- Administer high flow O2, consider need for intubation
- If stridor or upper airway obstruction, give inhaled epinephrine
- If wheeze or lower airway obstruction, give inhaled salbutamol
Hypotension or Decreased Level Of Consciousness (LOC):
- Supine position
- Secure large bore IV or obtain intraosseous (IO) access
- Crystalloid NS or LR , 20 mL/kg IV/IO rapid push
If no improvement, give 2nd dose of IM EPINEPHRINE
10 to 15 MINUTES
Respiratory symptoms:
- Repeat inhaled epinephrine (upper airway obstruction)
or salbutamol (lower airway obstruction) - Prepare for difficult airway intubation
Hypotension or Decreased Level of Consciousness (LOC), persistent abdominal pain/vomiting:
- 2nd crystalloid NS or LR, 20 mL/kg IV/IO rapid push
- Prepare for possible IV epinephrine infusion
If no improvement, give 3rd dose of IM EPINEPHRINE
ALERT Pediatric Referral Center
15 to 20 MINUTES
Respiratory symptoms:
- Consider 3rd inhaled epinephrine or salbutamol
- Consider IV hydrocortisone for persistent shock, asthma or upper airway obstruction
- Proceed with intubation if no improvement
Hypotension or Decreased Level of Consciousness (LOC):
- Start IV epinephrine infusion 0.05 mcg/kg/min IV, titrate up by 0.02 mcg/kg/min to effect
ALERT Pediatric Referral Center
REFRACTORY ANAPHYLAXIS
- Repeat boluses of Normal Saline (NS) 20 mL/kg
- Low Dose Epinephrine Push - 0.001mg/kg = 1 mcg/ml
- Norepinephrine infusion (For persistent hypotension):Start at 0.05 mcg/kg/min IV, titrate by 0.02 mcg/kg/min to effect (MAX 2 mcg/kg/min) until adequate perfusion
- Glucagon bolus (For persistent anaphylaxis symptoms or patients on beta blockers) Dose: 20 - 30 mcg/kg/dose (MAX 1 mg) IV over 5 minutes, followed by infusion of 5 -15 mcg/min, titrated to clinical effect
TREKK. Pediatric Anaphylaxis Algorithm [Internet]. 2025. Available from: Trekk - Anaphylaxis Algorithm.
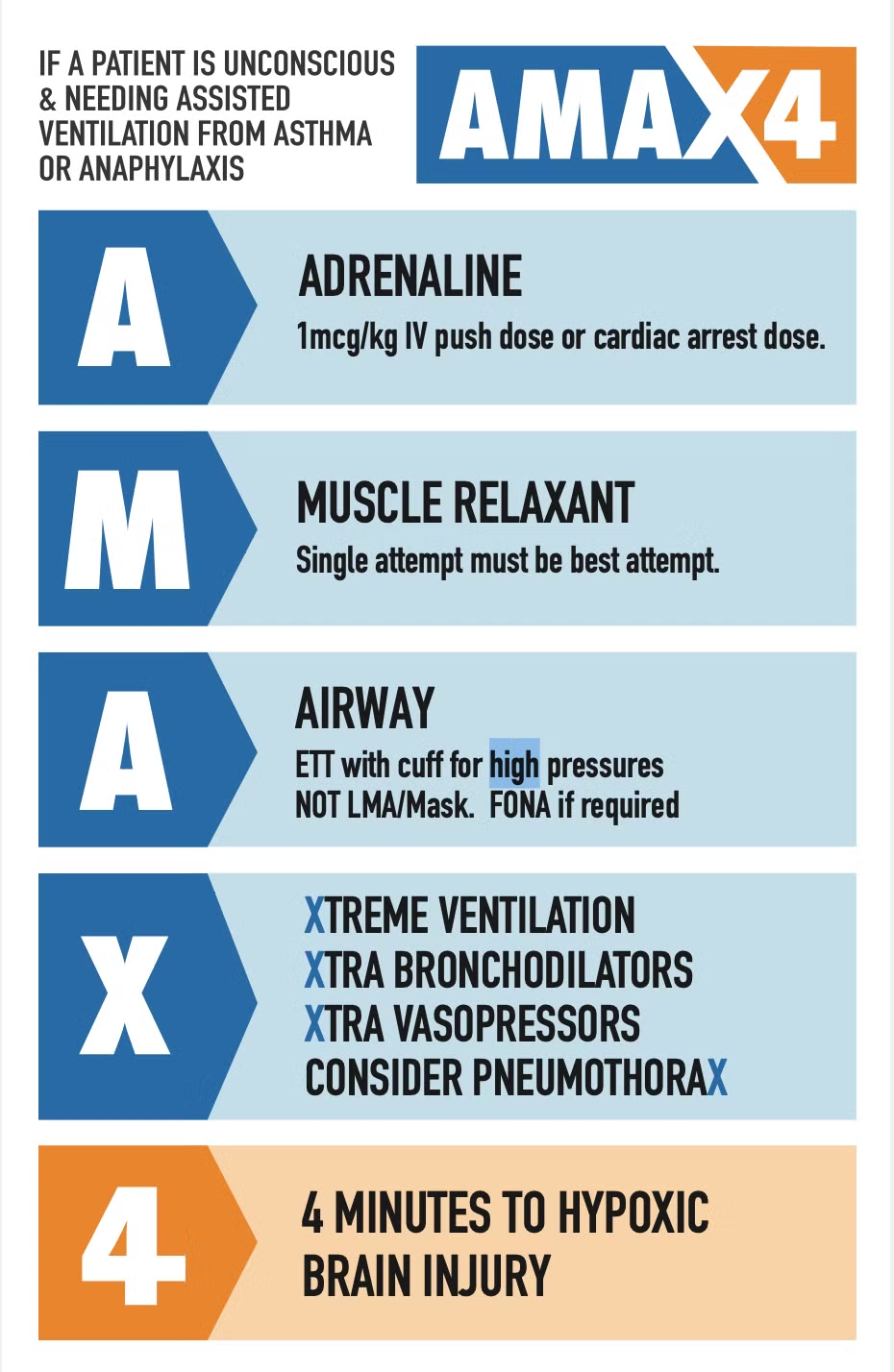
Ben and Tamara McKenzie. AMAX4 [Internet]. 2023. Available from: https://www.amax4.org/.